Cross-linking & topo-guided PTK
Cross-linking freezes progression; topo-guided PTK regularises the surface. Two complementary steps whose entire safety hinges on two numbers: 400 µm of residual stroma and a capped ablation.
Corneal cross-linking (CXL)
8.1 Principle
Riboflavin (photosensitiser) + UVA 370 nm → ROS generation → covalent cross-links collagen-collagen and collagen-proteoglycan → ↑ biomechanical rigidity and arrest of progression (≈ 90 % stabilisation). CXL stabilises without correcting: it does not restore vision, it prevents worsening.
8.2 Protocols
| Protocol | Parameters | Note |
|---|---|---|
| Dresden (standard epi-off) | Riboflavin 0.1 % (dextran) · 3 mW/cm² × 30 min | Reference Longest follow-up, maximum depth of effect. |
| Accelerated | 9 mW × 10 min · 18 mW × ~5 min · 30 mW × 3 min | Reciprocity law (Bunsen-Roscoe) with limits: lower depth efficacy at high intensity (oxygen-limited). |
| Iontophoresis / epi-on | Facilitated penetration without epithelial removal | Less penetrating/effective, but less morbid. |
| PACE / pulsed | Customised CXL, pulsed UV cycles | Improved stromal oxygenation. |
| Theranostic (iontophoresis) | Transepithelial, riboflavin delivered by iontophoresis; real-time monitoring of stromal riboflavin | The UV-A fluence is adapted continuously ("riboflavin score") → personalised, algorithm-driven dose. |
Theranostic CXL combines iontophoresis (transepithelial riboflavin delivery, epithelium preserved) with a "theranostic" UV-A device that measures stromal riboflavin concentration in real time (hyperspectral analysis, "riboflavin score") and adapts the UV-A fluence continuously — a personalised, algorithm-driven dose. Goal: to offset the poorer riboflavin penetration of transepithelial CXL and estimate cross-linking efficacy during the session. Evaluated in a randomised trial (ARGO protocol) with early one-year real-world data in progressive keratoconus.
8.3 Limits — to know by heart
- Minimum stromal pachymetry ≥ 400 µm after de-epithelialisation (endothelial protection against UVA). Thin corneas → hypo-osmolar riboflavin to swell to ≥ 400 µm, or epi-on/adapted.
- Keratometry: no strict safety threshold, but decreasing efficacy/predictability in very advanced cones (very high K max).
Cornea < 400 µm not swellable · corneal herpes (reactivation risk) · dense central scar · active infection · pregnancy (relative).
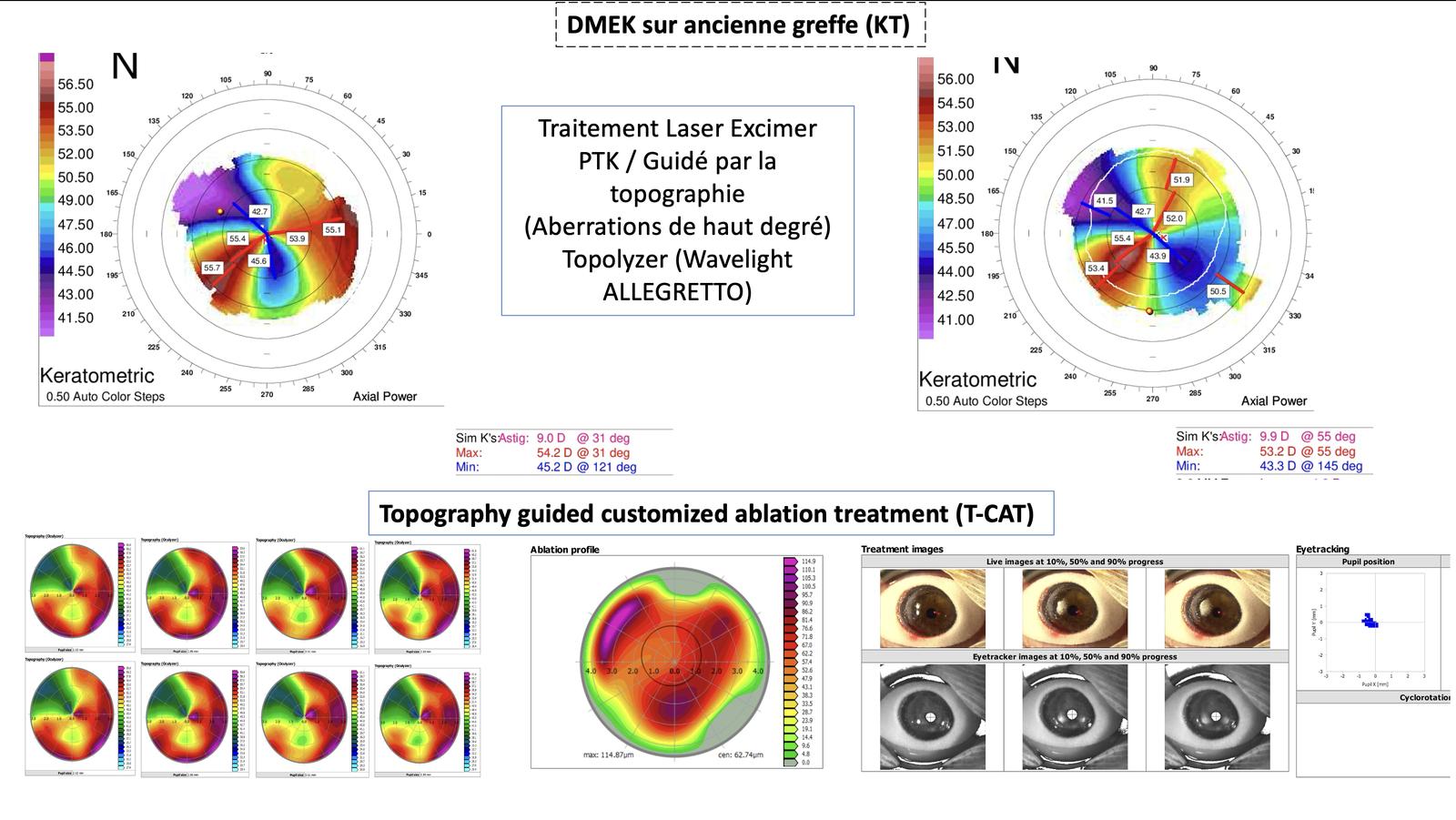
Topo-guided PTK ± CXL — combined protocols
9.1 Objective
Regularise the anterior surface (reduce irregular astigmatism and coma, improve acuity) — not correct the whole refractive error — while preserving tissue and combining with CXL so as not to destabilise.
9.2 Two ablation logics
- t-PTK (trans-epithelial, guided by the epithelial map): exploits epithelial remodelling; the epithelium acts as a smoothing "mask" — trans-epithelial ablation regularises by following the doughnut profile and paradoxically normalises the underlying stromal surface.
- Partial topo-guided PRK (Athens / Cretan-type protocols): myopic/topo-guided tissue-saving photoablation, capped.
9.3 Combined protocols
9.4 Stromal & keratometric limits — imperative
- Capped ablation depth: aim for ≤ 50 µm (regularisation goal, not full correction).
- Residual stromal bed ≥ 400 µm to allow safe CXL after ablation.
- Very steep cones (very high K max) = poor predictability; prefer stabilisation/ICRS over ambitious regularisation.
Never perform "full" topo-guided PRK on a keratoconus (risk of aggravated ectasia): always partial + CXL.
Illustrated clinical case — stepwise corneal regularization & IOL calculation
69-year-old woman, right eye. Cortico-nuclear cataract, keratoconus for 60 years, rigid contact lenses for 30 years. Work-up performed 4 months after lens discontinuation and 4 months after intracorneal ring segment (ICRS) implantation. The case illustrates a combined strategy: regularize the cornea (intracorneal rings, then topography-guided laser on higher-order aberrations), make IOL calculation reliable (total keratometry TK / EKR integrating the posterior surface), and manage an endothelial graft on an old keratoplasty.
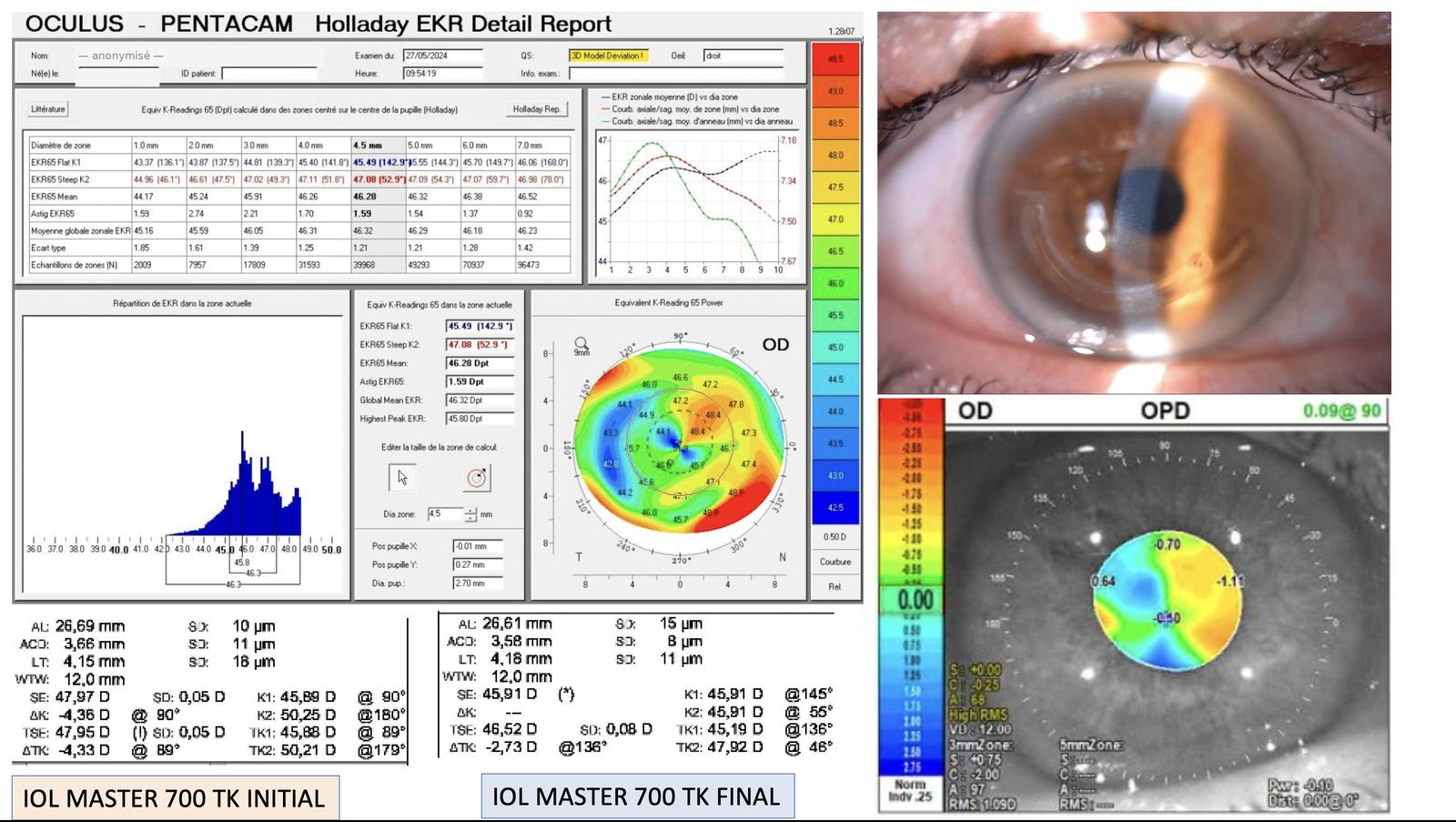
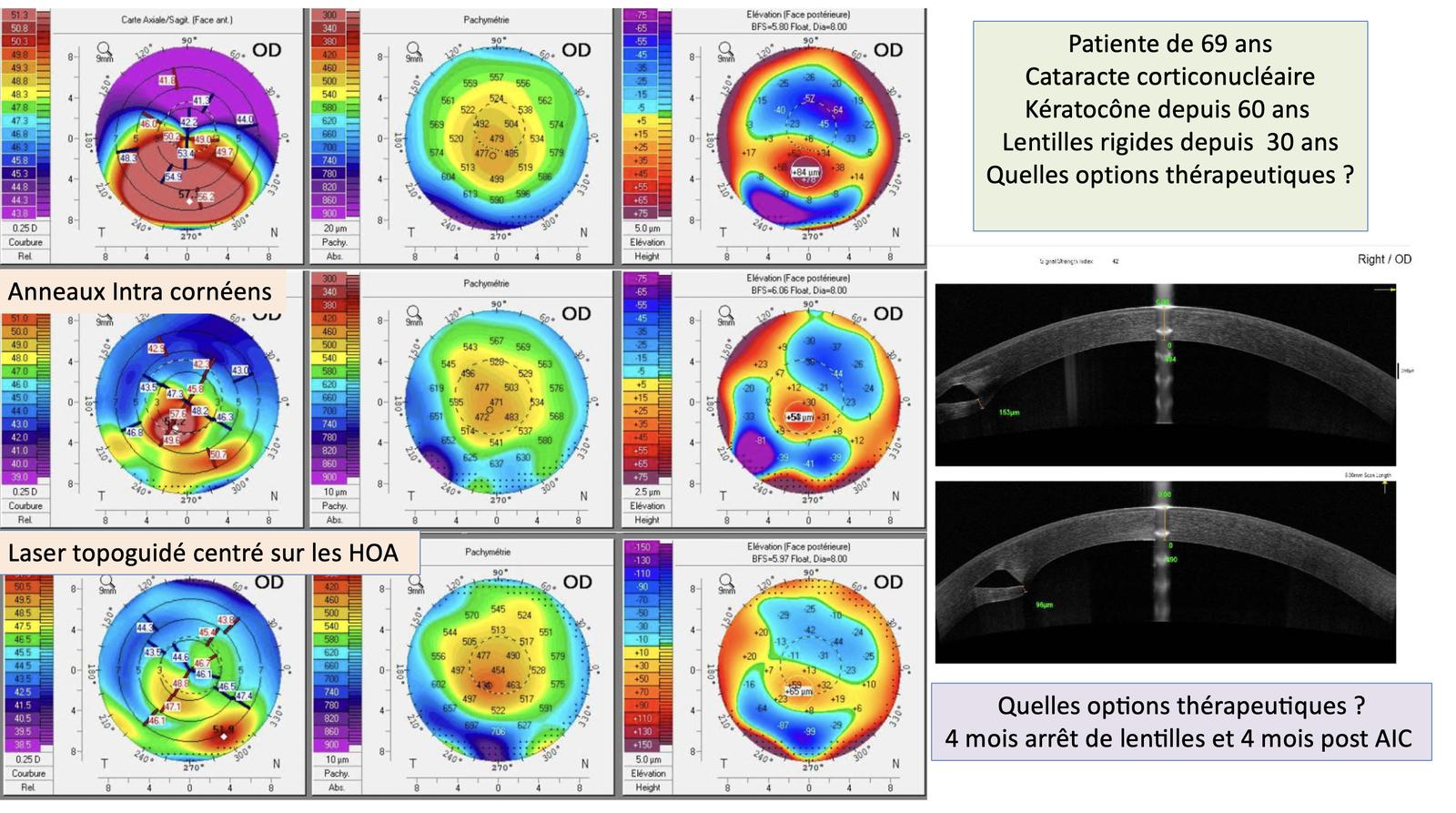
In long-standing keratoconus that develops a cataract, the sequence rings → topography-guided laser (T-CAT / PTK) → phaco with calculation on TK / EKR regularizes the irregular astigmatism and higher-order aberrations, makes IOL calculation reliable (total keratometry), and treats endothelial decompensation with DMEK even on an old graft. Regularize first, measure second.